

- Research: To support and guide comprehensive studies on dampness and mould, focusing on its health impacts and implications for building design. MAC’s goal is to contribute to a safer and healthier environment for everyone.
- Awareness: To educate and engage various stakeholders, including building professionals and medical practitioners, about the risks and consequences of dampness and mould exposure. By fostering a community of informed advocates, MAC aims to drive meaningful change.
- Recovery: To offer essential resources and support for those affected by mould-related illnesses, whether localized or systemic, acute or chronic. MAC aims to empower practitioners and individuals with the knowledge and tools needed to navigate and overcome mould-related challenges.
- Advocacy: To strive to provide much-needed credibility to the area of dampness and mould and its connections with health problems, to assist with the general perception of mould-related illnesses in the community, and to action policy change and develop an appropriate mould-related framework in Australia.
Fungi are a group of organisms that include:
- Moulds (filamentous fungi)
- Yeasts
- Mushrooms
Mould is a type of fungus that grows in multicellular filaments called hyphae, forming a fuzzy or powdery-looking colony. It thrives in warm, damp, and humid environments and reproduces by releasing microscopic spores into the air, which can settle on surfaces and spread where moisture is present.
Moulds also play an important role in nature by breaking down organic material like dead plants and animals. They have also been a source of many important medicines—including antibiotics, immunosuppressants, and statins. There is also renewed interest in the fungal byproduct psilocybin for use in depression and other psychiatric conditions. However, when mould grows indoors—especially in homes, workplaces, or buildings with water damage—it can become a serious health concern.
Mould is ubiquitous in the environment, and even the air we breathe contains fungal spores and fragments. In natural ecosystems such as forests, individuals typically do not fall ill from mould exposure in this context despite the high prevalence of species.
As such, few understand why mould in a water-damaged building represents a different exposure that can cause illness. However, in this context, specific species can dominate within the built environment, creating a unique exposure different to that found in nature.
Mould in nature:
- Mould is a natural part of the environment, functioning as a decomposer that breaks down organic material like leaves, wood, and dead animals.
- It exists in a balanced ecosystem, where it competes with other microorganisms and is naturally regulated by environmental factors such as sunlight, wind, and microbial competition and predators (including some insects).
- There is a tremendously diverse microbial ecosystem, of which moulds play a key role, which prevents pathogenic strains from becoming dominant.
- Outdoor air provides dilution, preventing mould spores from accumulating at high concentrations.
- Mould in natural environments typically does not pose a significant health risk unless there is an occupational exposure (e.g., working with compost, potting mix, or decaying wood in a closed space).
- Natural environments constantly degrade mycotoxins through UV exposure and diverse microbial activity. Indoors, the specific environmental stressors of a water-damaged building—such as limited, nutrient-poor substrates like drywall—trigger colonizing moulds to upregulate mycotoxin production as a survival mechanism, which then accumulate due to the lack of natural degradation.
Mould overgrowth in a built environment:
- In buildings, mould can become a problem when moisture levels rise due to leaks, flooding, condensation, or poor ventilation.
- Mould growth is often accompanied by a change in the types of bacteria living in the building. These bacteria have also been shown to cause significant adverse health effects. Mould is often the visible or odorous indicator of a harmful environment, but not the only health risk.
- Indoor environments lack the natural checks and balances found outdoors (such as UV light exposure, diversity in the ecosystem, and natural air circulation).
- Indoor environments can also includes unfavourable elements such as fungicides (which cause natural selection of more pathogenic moulds) and chemicals. Mould-food-rich conditions such as high levels of dust or cellulosic materials can allow mould to overgrow rapidly if climatic conditions are favourable.
- Mycotoxins and mould fragments which may contain toxins, allergens or other immune-impacting compounds can can become highly concentrated in enclosed spaces. Exposure to elevated levels of such microbial particles for long time durations can lead, leading to chronic exposure and potential health issues, especially for individuals with mould sensitivity, asthma, allergies, or mast-cell activation syndrome (MCAS).
- Indoor mould growth often involves species that thrive in damp, cellulose-rich environments (like gyprock, wood, and carpets), including Stachybotrys, Aspergillus, Cladosporium and Penicillium species, which can produce harmful mycotoxins.
- Mould and bacteria readily form biofilms when in contact with very wet surfaces. Biofilms are particularly hazardous as they encourage the development of greater microbial virulence, antimicrobial drug resistance and other protective microbial changes that increases the risk in the building.
In summary: Mould in nature is a critical regulator of the ecosystem, while mould in a built environment can become an unchecked health hazard.
Causes of mould in the built environment include excessive moisture in building materials and contents arising from:
- leaks
- floods
- storms
- condensation
- high humidity
However, the role of poor ventilation, build-up of general dust, dirt, and debris, and the lack of natural balancing factors such as beneficial microorganisms are often underestimated when solving or diagnosing mould problems in the building.
Mould-related illnesses represent a complex and emerging domain within medical literature. The physiological impacts of mould exposure are still being actively researched. Until recently, mainstream clinical medicine has accepted mechanisms of mould-induced pathogenesis: allergy, infection, and toxicity.
- Allergy (Atopy): Allergic responses to mould are driven by immune system hypersensitivity to fungal spores or hyphal fragments. Mould allergies can give rise to a variety of illnesses, primary affecting the respiratory system. Allergic responses can give rise to asthma and wheezing, particularly in children. Allergic rhinitis is also linked to allergic responses to mould as is hypersensitivity pneumonitis or “farmer’s lung”. Further, the condition known as allergic bronchopulmonary aspergillosis is related to a more severe allergic reaction to aspergillus species, leading to lung inflammation. Doctors will usually test for mould allergy via IgE blood tests or skin prick tests. Treatment is centred on exposure reduction and/or immunotherapy.
- Infection (Mycosis): This is where fungus reproduces on or in the human body. Fungal pathogens bypass the body’s physical barriers or evade immune clearance, leading to colonization, tissue invasion, and replication within the host. This can include mild, peripheral infections of the skin, hair, nails that are usually localised and non-life-threatening. However, systemic infection of the bloodstream or pulmonary infections within the lungs (e.g., invasive aspergillosis) can be life-threatening. Immunocompromised individuals are at higher risk of mycosis. Culture tests (sinus, nasopharynx, lungs), organic acids testing, and stool testing, and technologies such as qPCR and DNA sequencing can be used in the diagnosis of fungal infection. Subtypes include:
- Tinea: Fungal infection of the skin that causes itching and rashes. Usually treated by topical antifungals.
- Aspergilloma/cryptococcosis: This is when the mould Aspergillus (or the yeast Cryptococcus) causes fungal balls in the lungs. Symptoms include a cough bringing up blood, wheezing, shortness of breath, weight loss, and fatigue.
- Invasive aspergillosis/cryptococcosis: When the fungal infection from #2 spreads to the brain, heart, kidneys or skin, usually in people who are immunosuppressed, such as those having cancer chemotherapy/other immunosuppressant drugs, bone marrow transplantation, HIV, or other diseases of the immune system. Usually serious and, if untreated, can be fatal.
- Fungal meningitis: Similar to #3, but the fungus/yeast spreads to the areas around the central nervous system (e.g. brain or spinal cord).
- Candidiasis: An overgrowth of the yeast Candida. It can affect the skin, mouth, throat, vagina, and joints. Invasive candidiasis occurs when Candida spreads to the bloodstream creating a more serious illness. This is generally only diagnosed in immunocompromised individuals (e.g., those on chemotherapy or transplant immune suppressant medications).
- Toxicity (Alimentary Mycotoxicosis): Mycotoxicosis refers to a systemic pathology whereby mycotoxins produced by moulds are ingested from diet (i.e., mouldy food)—not from inhalation. There has been universal recognition by major public-health organisations such as the World Health Organisation (WHO) and US Food and Drug Administration (FDA) of the harms from ingesting excessive mycotoxins. Standards have been developed over decades to minimise mould and mycotoxin contamination of foodstuff, meaning that alimentary mycotoxicosis is now rarer in developed countries than it used to be.
These effects can be widespread, even affecting the central nervous system. There has also been some acceptance by mainstream medicine for toxicity caused by inhaled mycotoxins from occupational-related exposures where the acute level of exposure is incredibly high, although few mainstream practitioners are trained to recognise such exposures. Some of the specific effects of various mycotoxins include the following:- Ochratoxin A—Kidney damage, neurotoxicity
- Aflatoxins—Liver toxicity, increased cancer risk (hepatocellular carcinoma)
- Trichothecenes (e.g., T-2 toxin, DAS)—Neurological symptoms (e.g., headaches, brain fog, anxiety/depression, dizziness, vertigo, and peripheral neuropathy), respiratory and mucosal damage (including chronic sinus congestion, chronic cough, and irritation of the throat or eyes)
- Zearalenone—Estrogenic effects (eg triggering of oestrogen sensitive pathology such as fibroids or endometriosis), hormonal imbalances, reproductive issues
- Gliotoxin—This can cause gastrointestinal and microbiome disruptions, neurological symptoms (eg fatigue, brain fog, mood disturances and peripheral neuropathy) and respiratory and sinus-related issues.
Scientific evidence for other forms of illness from mould exposure are now emerging with varying acceptance. In addition to the aforementioned mechanisms accepted by mainstream medicine, of note are the following:
- Innate immune activation (CIRS): While the innate immune response is intended to be a short-lived immune response heralded by the production of cytokines, in mould-related innate immune activation, it persists as the dominant immune response resulting in persistent inflammation and release of cytokines. These cytokines are released by various white blood cells in the systemic circulation and by activated microglia in the central nervous system. The result is a systemic inflammatory response, similar to that described as “chronic inflammatory response syndrome” (CIRS) by Dr Ritchie Shoemaker & colleagues. This mechanism is primarily associated with the lower, chronic (ongoing) exposure to dampness and mould that can occur in water-damaged buildings.
While there is no formal acceptance for the CIRS case definition of mould illness, the US National Institutes of Health do recognise innate immune activation as the likely mechanism causing cognitive issues, inflammatory immune effects, and mental-health problems. - Microbiome dysbiosis: Sometimes incorrectly described as fungal colonisation, this health problem is different to fungal infection (mycosis) in mainstream medicine. In such instances, the gastrointestinal tract, nasal and/or sinus cavities can be colonised with a disproportionate amount of various fungal species (typically yeasts, including Candida), which can lead to adverse health effects. Critically, while bacteria and yeasts are common in the gut microbiome, moulds are usually only transient in healthy individuals and cannot survive at human body temperature (37 degrees Celsius). As well, microbiome dysbiosis can occur in individuals who are not immunosuppressed.
Symptoms may be single system (localised to the system of dysbiosis), or, if the fungus is producing mycotoxins or inflammatory proteins, multisystem. Treatment usually involves antimicrobials to reduce the fungal burden and pro/pre-biotics to improve the terrain, but binding and inflammation-reduction therapies are often used in conjunction. While mainstream medicine increasingly recognises emerging science that shows an important role of the gut microbiome in human health, few mainstream practitioners yet diagnose or treat the condition. - Inhaled toxicity (Mycotoxicosis): Like alimentary mycotoxicosis that can occur from eating (ingesting) mould and mycotoxins from food, some integrative/functional practitioners believe that inhaled mycotoxins breathed in from the air are sufficient to cause toxic effects in the body. There is currently debate even withing integrative/functional medicine as to what proportion of effects from inhaled mycotoxins are caused by toxicity as opposed to innate immune activation (or CIRS). Not all practitioners within integrative/functional medicine agree that inhaled myotoxicity can occur, believing the dose to be too low, instead attributing adverse health effects primarily to innate immune activation.
- Ritchie Shoemaker, MD / Andrew Heyman, MD:
- Dr Shoemaker from Pocomoke City, Maryland in the US is the primary researcher for the Center for Research on Biotoxin-Associated Illness. Shoemaker stumbled across what he would later coin biotoxin-related illness in the late 1990s due to a pfiesteria outbreak on the Chesapeake Bay. In the early 2000s, he published studies showing that biotoxins from water-damaged buildings (then called sick building syndrome) caused a similar type of syndrome that he later labelled CIRS-WDB. This stands for “chronic inflammatory response syndrome due to exposure of the interior of water-damaged buildings”. He developed a series of biomarkers to look at the inflammatory changes that occur in this illness, which is primarily related to mould and bacteria such as actinobacteria. His primary treatments include removing patients from further exposure, cholestyramine and colesevelam as biotoxin binders, EDTA nasal spray, and a nasal spray of vasoactive intestinal polypeptide (VIP).
- Dr Heyman from Aldie, Virginia in the US also follows a CIRS-focused approach to treatment, but adds additional supplements prior to and during treatment.
- Neil Nathan, MD / Jill Crista, ND:
- Drs Nathan and Crista have a holistic medicine approach for systemic mould-related illnesses, aligning primarily with the microbial dysbiosis and inhaled mycotoxicosis subtypes of mould illness. Nervous system dysregulation plays a huge role in chronic illness, and rebooting the system can be a key part of recovery. As such, Drs Nathan and Crista utilise multiple avenues such as brain retraining and vagal stimulators to assist with rebooting the nervous system. They also address mast cell activation as a primary mechanism for mould-related inflammation.
For diagnosis, they primarily use urinary mycotoxin testing and their treatment involves targeted binders based on which mycotoxins are elevated. If sinus/nasal fungal colonisation/dysbiosis is diagnosed, then antifungal medications (Dr Nathan) or herbs (Dr Crista) are prescribed intranasally, while oral antifungal medications (Dr Nathan) or herbs (Dr Crista) are often used for gastrointestinal dysbiosis. They may also use multiple other therapies, including ozone therapy plus phosphatidylcholine and other membrane stabilisers. - While Dr Nathan uses binders and some of other CIRS treatments, Dr Crista focuses more on toxin drainage, herbal antifungals, and bioflavanoids.
- Drs Nathan and Crista have a holistic medicine approach for systemic mould-related illnesses, aligning primarily with the microbial dysbiosis and inhaled mycotoxicosis subtypes of mould illness. Nervous system dysregulation plays a huge role in chronic illness, and rebooting the system can be a key part of recovery. As such, Drs Nathan and Crista utilise multiple avenues such as brain retraining and vagal stimulators to assist with rebooting the nervous system. They also address mast cell activation as a primary mechanism for mould-related inflammation.
- Andrew Campbell, MD:
- Dr Campbell is a Mexico-trained MD who primarily ascribes mould-related illness to be due to mycotoxins and microbiome dysbiosis. His preferred testing is serum mycotoxin antibodies done via the laboratory MyMycoLab, of which he is the medical director. His treatment protocol does not use binders; instead, he uses the pharmaceutical antifungal itraconazole orally, plus various natural supplements such as vitamin D and B complex, vitamin C, Omega 3s, CoQ10, melatonin, and spore-based probiotics.
All of the main thought leaders advocate removing the patient from further exposure to environmental dampness and mould as the most important step in recovery. While Shoemaker protocol currently focuses more on bacteria (actinomycetes) in the environment, these co-exist hand-in-hand with dampness and mould in most cases.
Two out of the three major protocols (Shoemaker & Nathan) include the use of binder medications and/or supplements, and two of the three major protocols (Nathan & Campbell) include use of antifungal therapies (pharmaceuticals and/or herbal antifungals).
All the protocols involve some form of therapy to reduce inflammation whether it be pharmaceutical (Shoemaker) or a combination (Nathan) or primarily natural supplement-based (Campbell).
Only CIRS-focused protocols attempt to diagnose and treat potential neurological atrophy observed in some (but not all) cases of systemic mould-related illness.
A summary of an integrated protocol might look like this:
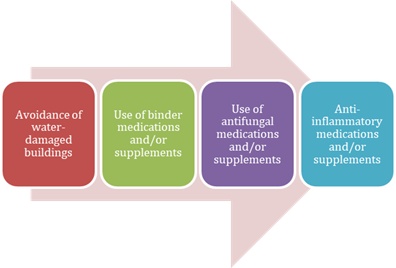
© Mold Illness Mastery course
For microbiome dysbiosis and inhaled mycotoxicosis, yes, mould, yeast, and their byproducts (e.g., mycotoxins) are the cause.
However, innate immune activation may be caused by the toxigenic microbial soup found in water-damaged buildings and includes mould fragments, mycotoxins, mannans and beta-glucans from mould, endotoxins and exotoxins from bacteria (including gram positive and gram negative bacteria, mycobacteria and actinobacteria), microbial volatile organic compounds (mVOCs) from bacteria and mould, VOCs from building materials that are broken down through microbial activity, and many more compounds. Mould is just the most visible, most researched and easiest microbe to test for.
Recently, CIRS-focused research has identified actinomycetes as a predominant cause of systemic mould-related illness. However, little independent research exists to confirm this association.
Common conditions that mould-related illness is associated with include:
- Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)
- Fibromyalgia
- Multiple Chemical Sensitivity (MCS)
- Inflammatory Bowel Disease (IBD), Irritable Bowel Syndrome (IBS), SIBO, Leaky Gut (webinar)
- Alzheimer’s disease (webinar)
- Parkinson’s disease
- Mast Cell Activation Syndrome (MCAS) (webinar)
- Multiple Sclerosis (MS)
- Depression and mental-health issues (NIH)
- Post Traumatic Stress Disorder (PTSD).
Please see the MAC Medical Testing page for in-depth testing details and links.
The VCS is a simple visual test used to screen patients to see if they are affected by biotoxins/toxicants, as these cause inflammation that results in hypoperfusion (lack of blood flow) throughout the optic nerve. The test measures your ability to distinguish between finer and finer increments of light versus dark (contrast).
Further details of the VCS test can be found on the Medical Testing page.
A summary of relevant blood markers are presented in the table below.
| BIOMARKER | AUS LAB (NATA) | MEDICARE | FASTING | RANGE (Shoemaker) | NOTES |
|---|---|---|---|---|---|
| α-MSH | N/A | 35-81 pg/mL | |||
| ACTH | Local lab | Y | Interpret with cortisol | ||
| Anti-gliadin antibodies | Local lab | Y | 0-19 (IgA, IgM) | Sometimes elevated in CIRS | |
| Anti-phospholipid antibodies | Local lab | Y | 0-12 (IgA), 0-10 (IgG), 0-9 (IgM) | Sometimes elevated in CIRS | |
| C4a | N/A | 0-2830 ng/mL | |||
| Copectin (ADH surrogate marker) | Local lab -> RPA | N - Out of pocket cost varies | 1.0-13.3 pg/mL | NSW Health Pathology page | Common pattern is low copeptin with high osmolality | |
| Cortisol (AM) | Local lab | Y | Pattern can be low ACTH and low cortisol but sometimes high ACTH, high cortisol | ||
| DHEA | Local lab | Y | Sometimes low in CIRS | ||
| Estradiol | Local lab | Y | Sometimes high in CIRS | ||
| HLA DR/DQ | Sonic Group or NutriPATH | Y (66695) | Sonic page | ||
| Leptin | Local lab -> RPA | N - Out of pocket cost varies | Y | NR 2-5.6 ng/mL (M), 3.7-11.1 ng/mL (F) | NSW Health Pathology page |
| MMP-9 | N/A | 85-332 ng/mL | |||
| Serum Osmolality | Local lab | Y | 280-300 mmol/kg | Interpret with ADH | |
| Testosterone | Local lab | Y | Sometimes low in CIRS | ||
| TGF-β1 | N/A | 344-2380 pg/mL | |||
| VEGF | Local lab -> Peter MacCallum Cancer Centre | N - Out of pocket cost varies | 31-86 pg/mL | Transport on ice / store refrigerated | Only performed infrequently | |
| VIP | Local lab -> RPA | Y (71151) | Y | 6.8-18.6 pmol/L | NSW Health Pathology page |
See the Medical Testing page for in-depth information.
NutriPATH offers biotoxin/mould blood panels that test many of the core CIRS biomarkers. However, apart from HLA DR/DQ genetic testing and the MARCoNS nasal swab, these tests cannot be recommended at this time due to inaccuracies compared to US laboratories.
(These inaccuracies were discovered by Dr Sandeep Gupta, who compared biomarker testing from Quest Diagnostics against NutriPATH’s results. Ref: Mold Illness in Children webinar (35m) and Low Tox Life podcast episode 55.)
No other accurate Australian diagnostic testing for TGF-b1, C3a, C4a, MMP-9, and MSH is currently available. (However, testing for VIP and VEGF is available from other Australian pathologies.)
2.4.1 What is the HLA DR/DQ Genetic Test (a.k.a. Mould Genes)?
In unpublished research conducted by Dr Shoemaker of his 10,000-size patient population, approximately 25% of the general population have Human Leukocyte Antigen (HLA) genes that are mould, Lyme or multi-susceptible (i.e., susceptible to toxins from mould/WDB, Lyme, and dinoflagellates). Dr Shoemaker’s hypothesis is that when these genes are primed (see 2.4.5) and a person is exposed to a high level of toxins/toxicants from water-damaged buildings, the immune system does not make the appropriate antibodies to clear them due to a defect in antigen presentation, which creates a state of chronic inflammation and upregulation of the innate immune system.
Critically, this research has not yet been replicated. While there may be a role for the HLA system in antigen presentation of biotoxins, further research is needed to establish such a link.
Note: The HLA genes merely indicate a potential genetic susceptibility to CIRS and having them does not automatically mean you have/or will develop CIRS.
2.4.2 My partner/child has HLA-susceptible genes but they don’t get sick with exposure to water-damaged buildings. Why is this?
Dr Shoemaker found that HLA genes generally need to be primed by an inflammatory illness, or event, that causes a cytokine storm. Possible priming events include influenza, Coxsackie virus, Lyme disease, mononucleosis (Epstein Barr Virus/glandular fever), ECHO virus infections, intense inflammatory lung responses, and unusual conditions such as Kawasaki disease. (Berry, 2014, p14). In 2021 Shoemaker et al published a paper that a small cohort (n=21) of Post COVID Syndrome (a.k.a. Long COVID) patients shared proteomic (blood protein) similarities to CIRS patients.
However, if there is a great deal of inflammagens, biotoxins and toxicants in a water-damaged building that can be enough to prime the genes and cause CIRS by itself.
2.4.3 Getting the HLA gene test in Australia
Further details on how to get the HLA DR/DQ genetic test are on the Medical Testing page.
2.4.4 Does 23andme or similar genetic testing show these HLA genes?
No. 23andme does not show all the HLA haplotypes and not in a format that correlates to Dr Shoemaker’s table.
2.4.5 HLA susceptibility in other disease states
MAC staff have put together a Google spreadsheet that summarises many disease susceptibilities, and also disease protection, corresponding to Dr Shoemaker’s HLA haplotypes found in the scientific literature. Autoimmune conditions in particular are prevalent.
NeuroQuant® is a software program from Cortechs Labs that measures microscopic volumetric changes in defined areas of the brain from a magnetic resonance imaging (MRI) scan. Dr Shoemaker’s research found microscopic interstitial oedema, a.k.a. neuroinflammation, and atrophy, a.k.a. neuronal loss, in brain areas in two small studies (2014, 2017) of CIRS patients. Additionally, Professor Dale Bredesen also published a paper (2016) on a case series of patients suffering an early-onset form of cognitive decline he dubbed “Inhalational Alzheimer’s Disease”, which involved a subset of CIRS patients.
A limitation of volumetric MRIs is that it cannot show the volume of the brain before the illness. However, NeuroQuant can also be a tool to track inflammatory and atrophic changes at baseline and throughout treatment. Successful treatment can sometimes demonstrate the reversal of neurological atrophy.
Further details on obtaining a NeuroQuant scan are on the Medical Testing page.
Multiple Antibiotic Resistant Coagulase Negative Staphylococci (MARCoNS) are bacteria that colonise the nasopharynx area forming biofilms and creating exotoxins. The underlying research was based on studies associating membrane-damaging toxins from coagulase-negative staphylococci that colonised the sinuses with chronic orofacial muscle pain (1998).
MARCoNS form due to low levels of MSH in mucous membranes, which is antimicrobial and anti-inflammatory. MARCoNS can themselves further lower MSH levels. Dr Shoemaker reports MARCoNS colonisation in 80% of CIRS patients, although further research is needed to replicate these results.
See the Biotoxin pathway diagram to see how hormones and immunity are affected in CIRS.
- Berry, Y. (2014). A physician’s guide to understanding & treating biotoxin illness. Surviving Mold.
- Shoemaker R, Lipsey R. (2006). Results of health screening and visual contrast testing. St. Bernard’s Parish, Louisiana. Surviving Mold. Full-text
- Shoemaker R., McMahon S, Heyman, A., Lark, D, van der Westhuizen, M., & Ryan, J. (2021).Treatable metabolic and inflammatory abnormalities in Post COVID Syndrome (PCS) define the transcriptomic basis for persistent symptoms: Lessons from CIRS. Medical research archives, 9(7). https://doi.org/10.18103/mra.v9i7.2493
Urinary mycotoxin tests detect metabolites (breakdown products) of mycotoxins that your body has processed and excreted in urine. They are mostly used as a screening test for mould exposure, but can also be used as a diagnostic tool when used alongside clinical history, symptom analysis, building inspection and other tests (e.g. VCS test, HLA gene test etc).
Two laboratories, Realtime (available via NutriPATH) and Mosaic (formally Great Plains, available via RN Labs) currently offer urine mycotoxin testing in Australia.
See the Medical Testing page for details of how to order these tests, along with relevant research studies.
His company MyMycolab provides testing of IgG and IgE antibodies of 12 different types of mycotoxins in blood serum. Based on his prior published research, he believes the IgE response occurs when there is a large exposure to that particular mycotoxin and has mast cell involvement, while IgG responses are indicative of lesser amounts of exposure. Unlike antibodies to mould spores, mycotoxin antibodies are short lived and should reduce after 6 months of avoiding exposure.
This test can be ordered and drawn by those in Australia and shipped back to the US via FedEx. See the Medical Testing page for more details, including research studies, on this test.
Organic acids are chemical compounds excreted in the urine of mammals that are products of metabolism. The Organic Acids Test (OAT) offers a comprehensive metabolic snapshot of a patient’s overall health with 76 markers. When elevated, markers 1-9 can indicate yeast and fungal overgrowth/colonisation in the GI tract. Elevations of markers 10-18 can indicate bacterial overgrowth.
Two laboratories, Realtime (available via NutriPATH) and Mosaic (formally Great Plains, available via RN Labs) currently offer urine Organic Acids Testing in Australia.
See the Medical Testing page for details of how to order these tests.
Nasal/sinus testing:
- Swab or mucus sample from deep nasal passages or sinuses
- Ideally collected by an ENT via endoscopy
- Can also access a nasal swab via NutriPath (Code 3418)
- Can detect mould species like Aspergillus and Penicillium
- Main types of analysis are nasal culture and PCR
Sputum/lung testing:
- Used when there is a chronic cough, asthma-like symptom and/or suspected fungal lung involvement
- Main types of analysis are sputum culture and PCR
Mould allergy testing tests for an IgE allergic reaction to certain species of mould spores. Tests are often not specific to a single species of mould but a mould mix, and also not to mycotoxins. This testing is usually done via skin prick testing or blood RAST testing. As this is a common test, many different Australian laboratories offer it, and it is covered by Medicare. It is often the only mould-related test many GPs or allergists will know of and believe to be worth doing.
The problem with such testing, however, is that mould allergy is an adaptive immune system antibody response and is different from CIRS, which is a chronic innate immune system response. It is possible, but not that common, to have both mould allergy and CIRS.
ArminLabs in Germany, known for their Lyme (Borrelia) and co-infection testing, also offer EliSpot testing for Aspergillus Peptide Mix 1 & 2. This tests for the cell-mediated, rather than the humoral (antibody), arm of the adaptive immune system. This may be more relevant than standard mould allergy testing, as it can detect when T-cells release cytokines in response to Aspergillus and may give a clearer indication of whether there is chronic inflammation occurring in response to mould exposure.
Reducing or, ideally, eliminating exposure to mould and other biotoxins/toxicants from water-damaged buildings is the first step in any treatment protocol for any kind of mould-related illness. Before spending money on any other form of treatment, patients need to avoid the source of their illness. While this step is of paramount importance, it is often the most difficult, because places of residence (home), work, education (school, university), and even vehicles all need to be considered. These locations and vehicles will need to be either adequately remediated (which can be costly), or the patient will need to relocate to a safer environment or replace the vehicle.
Many Mould Illness patients develop an environmental sensitivity, whereby they react to even small amounts of biotoxins and toxicants in water-damaged buildings and vehicles. Some of the most extreme reactors often resort to camping in dry locations in tents, caravans (RVs), or converted trailers. Patients monitor how their symptoms fluctuate to deduce what locations or (potentially) even possessions are exacerbating their illness.
This form of extreme mould avoidance originated with Erik Johnson, who was a prototype for chronic fatigue syndrome during the original outbreak of the syndrome around Lake Tahoe, Nevada in the mid-1980s. Erik became largely symptom free with using extreme mould avoidance. For more on Erik’s story and mould-avoidance techniques, please read Back from the edge by Lisa Petrison (see resources).
The use of binding medications or supplements to adsorb mycotoxins and other toxins/toxicants in the intestines is suggested by most Mould Illness practitioners, except for Dr Andrew Campbell and those strictly following his protocol.
Side-effects
Binders can have some gastrointestinal (GI) side-effects such as constipation, gas, and acid reflux. Constipation can usually be ameliorated with magnesium citrate, vitamin C, and/or soluble fibre (chia seeds, flax seeds, and psyllium). Long-term use of binders can deplete fat soluble vitamins (A, E, D, K, CoQ10), so many practitioners suggest to supplement these, taking them at a different time of day to binder dosing.
How long do I stay on binders?
This is highly individualised but typically varies between three and twelve months. Duration of binder use is dependent on improvement in lab work, symptom reduction, and absence of exposure to further water-damaged buildings.
Some people stay on a lower maintenance dose of binders on a continual basis, or increase them short term when re-exposed to a water-damaged building (e.g., take a full dose for 3–7 days after exposure).
Worsening of symptoms (intensification reaction)
Dr Shoemaker hypothesised that binders, especially cholestyramine, can cause an intensification reaction (a general worsening of symptoms)—commonly but incorrectly referred to as herxing/herx—especially in Lyme patients. This is because as biotoxins detach from cell receptors, they can enter the bloodstream and cause a rise in inflammatory cytokines.
Symptoms will generally be exacerbated, along with a worsening of visual contrast sensitivity (in columns D and E). The protein biomarker MMP-9 will also increase.
Dr Shoemaker suggests an inflammatory-lowering mini-protocol using fish oil. Start at least ten days before starting cholestyramine. If symptoms intensify, either lower or stop the cholestyramine dose, and then follow the interventions below for 5–10 days before restarting.
- No-amylose diet:
- A no-amylose diet enhances the effectiveness of Actos or fish oil.
Amylose is found in most grains, vegetables grown below the ground (root vegetables), and bananas. Similar diets include low carbohydrate, grain free, paleo diets such as the Bulletproof diet, Wahls Diet, or Doug Kaufman’s Phase I diet for at least the duration of CSM treatment.
- A no-amylose diet enhances the effectiveness of Actos or fish oil.
- High-dose fish oil:
- High-dose fish oil can lower inflammatory cytokines and other inflammatory markers. Dr Shoemaker suggests a dose of fish oil where the daily total of EPA at least 2.4 grams per day and DHA is 1.8 grams for ten days, with cholestyramine started on day six. Many people stay on this high-dose fish oil for longer.
Two pharmaceutical binders are available by presciption only.
Cholestyramine (CSM)
Cholestyramine (CSM) is a sixty-year-old cholesterol lowering medication that has been extensively studied with a good safety profile. This negatively charged binding resin attracts positively charged toxins/toxicants from bile and excretes them in the faeces. It is not absorbed systemically but only passes through the gastrointestinal tract. CSM is available in Australia either as Questran Lite, which contains aspartame, or as a pure compounded version. The compounded version may contain stevia and various forms of cellulose, which are harmless excipients for most people. (See resources for compounding pharmacies.) The full dosage is four grams four times per day (QID), thirty minutes before meals/medications or one-two hours after meals/medications. Many clinicians suggest starting with a small dose (1–4 grams) and working your way up to the full dose.
CSM is the only binder tested in clinical trials in humans that demonstrates efficacy in lowering associated inflammatory biomarkers.
Colesevelam (Welchol)
Colesevelam (brand name Welchol) is a medication similar to CSM. It generally causes less GI side effects, and can be taken with food. It is the binder recommended by Dr. Shoemaker for sensitive patients who can’t tolerate CSM. One caveat is that colesevelam only has 25% of the binding capacity of CSM. Like CSM, colesevelam can only be obtained at a select number of compounding pharmacies in Australia. Dosage is two tablets (625mg) up to three times per day.
Non-systemic binders (these stay in the GI tract)
- Activated charcoal—A broad spectrum binder that has been used successfully in animal mycotoxin and endotoxin (bacterial toxin) studies. It can also bind pesticides and VOCs but may bind with nutrients so, as with CSM, activated charcoal is best taken away from other supplements and medications. Suggested dose: 500–1000mg, 2–4 times per day. Suggested brands: Bulletproof, Blants (powder form) and Nature’s Way. Caveat: it will cause darkening of stools.
- Chitosan—Similar in structure to CSM and Welchol, Chitosan has a similar effect to those medications of lowering cholesterol, but it may also have anti-microbial and anti-cancer properties. Caveat: Derived from shellfish. (1, 2, 3). Suggested dose: 500–1000mg, 2–4 times per day. Suggested brands: Now, Nutricology, and Natural Balance.
- Bentonite clay (aka montmorillonite)—Binds to mycotoxins (1, 2), bacterial toxins (1, 3), pesticides (1), and heavy metals (1). Suggested dose: 1–3 grams, 2–4 times per day. Suggested brands: Blants, also widely found on eBay (make sure it is marked for human consumption/internal use).
- Zeolite clay (aka clinoptilolite)—Similar to bentonite clay. Established as a mycotoxin binder in animal studies (1, 2, 3). Suggested dose: as per bentonite. Suggested brands: Vita Pure (LavaeVitae), Zeolith MED, Toxaprevent, ZeoBind (BioPure)
Systemic (these are absorbed into the blood stream)
- Nanoised zeolite—This is a form of zeolite small enough to be absorbed into the blood stream and cells from the gut. As with normal zeolite, it is mainly thought of as a heavy metal chelator. (No peer reviewed studies are found for nanoised zeolite and chelation or binding; refer to zeolite research above.)
- Modified citrus pectin—A fibre from citrus peel that is known to bind to heavy metals (especially lead) and environmental toxins. It also has anti-cancer/anti-galectin 3 effects. Brands include Pectasol-C and Now (among others). (1, 2, 3, 4).
- Glutathione—The body’s master antioxidant. It can also aid in the detoxification of toxins including mycotoxins, and heavy metals. Gluthathione can be used in various forms including liposomal, intravenous, intranasal, N-acetylcysteine (a precursor) and L-glutathione.
Combination formulas
- Ultra Binder (Quicksilver Scientific)—This formulation combines bentonite clay, activated charcoal, chitosan, aloe vera, zerolite, and acacia gum.
- GI Detox (Biocidin Botanicals)—This formulation combines zeolite clay, activated charcoal, aloe vera, apple pectin, silica and humic powder.
- Shoemaker, R. C., & House, D. E. (2006). Sick building syndrome (SBS) and exposure to water-damaged buildings: time series study, clinical trial and mechanisms. Neurotoxicology and teratology, 28(5), 573-588. PMID 17010568
- Shade et al. (2018). A Push-Catch System That Enables Effective Detoxification. The Townsend letter, February/March 2018. Link.
- Huwig, A., Freimund, S., Käppeli, O., & Dutler, H. (2001). Mycotoxin detoxication of animal feed by different adsorbents. Toxicol Lett, 122(2):179-88. PMID 11439224
- Wilson, T. (2017). Are you detoxing with the correct binders. Sophia Health Institute. Link.
- Rudd, C. (2024). The Binder Compendium. Google doc.
A popular treatment protocol for Mould Illness (CIRS) is the Shoemaker Protocol, named after its originator, researcher Dr Ritchie Shoemaker. This is an eleven-step protocol designed to restore immune homeostasis. Parts, but not all, of this protocol have been trialled in published studies on CIRS, unlike some other Mould Illness protocols.
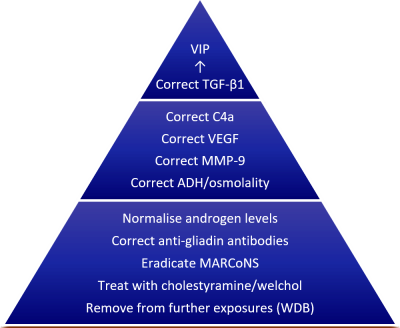
Shoemaker Protocol (© R. Shoemaker)
According to the Shoemaker Protocol, after removal from mould exposure/WDBs and at least one month of binders, MARCoNS should be treated if tested positive.
- Current Recommended Treatment—EDTA plus colloidal silver nasal spray
- If positive for MARCoNS, a patient will be begin a nasal spray of EDTA/colloidal silver nasal. EDTA helps break down the biofilm and the colloidal silver is an effective antimicrobial with some anti-biofilm activity as well. The duration of this treatment can be between one and several months.
- Past Treatments
- Previously, BEG nasal spray was used which contained Bactroban, EDTA, and Gentamicin. With the increase of antibiotic resistant MARCoNS strains and studies done by Dr Joseph Musto of Microbiology DX showing the effectiveness of colloidal silver, the protocol has been changed.
- Alternative treatments
- Neti pot or nasal spray of water with iodine or salt or xylitol (e.g. xyclear).
- Colloidal silver nasal spray by itself may help.
- Nebulised PVP-iodine may be effective according to Greg Muske of Biotoxin Journey. Read his detailed MARCoNS, More MARCoNS, and Even more MARCoNS blog posts for more details.
- Follow up testing
- After one to several months of treatment, patiensts should repeat the MARCoNS test. If still positive, consult with your health practitioner for treatment options.
After removal from WDB exposure, pharmaceutical binders, and treatment of MARCoNS, patients will undertake a number of mid-level steps aimed at both reducing inflammatory biomarkers and restoring affected hormones to normative levels.
Vasoactive Intestinal Polypeptide (VIP) is a neuropeptide hormone that is predominately made in the hypothalamus. Along with MSH, VIP is critical in controlling inflammation and the immune system. In a 2013 study and in clinical practice, Dr Shoemaker found that VIP:
- Increased plasma VIP levels
- Reduced symptoms to the level of healthy controls
- Reduced inflammatory cytokines (TGF-b1, C4a, MMP-9)
- Increased VEGF
- Balanced Treg immunity
- Increased 25-Vitamin D levels
- Normalised low testosterone levels in Males
- Normalised high estradiol (estrogen) levels in Males
- Increased tolerance to water-damaged buildings
Intranasal VIP has also been shown in a small clinical trial and case studies to correct multinuclear atrophy of grey matter in the brain, although further research is needed to confirm these findings.
However, the caveat to VIP therapy is that if you’re still being exposed to biotoxins from water damaged buildings or MARCoNS, then instead of reducing inflammation—such as TGF-b1 and C4a—VIP can potentially increase it. Thus, the following conditions must be met before using VIP spray.
- You live, work, and study in buildings with a HERTSMI-2 score of < 11
- You pass the VCS test
- You test negative for MARCoNS
- You have normal lipase levels.
My VIP level is normal, can I still benefit from VIP spray?
Yes. VIP has wide ranging effects apart from repleting VIP plasma levels. If you still have symptoms even with a normal VIP level, VIP may help.
Removal from mycotoxin exposure is the the first step to deal with mycotoxin toxicity. Both via removal from exposure to water-damaged buildings and/or reduction of internal fungal colonisation.
Most practitioners, except for Dr Andrew Campbell, suggest that binding supplements/medications are also needed to bind (adsorb) mycotoxins in the GI tract after being released in the bile. See Part 4.3-4.5 above for more information on this.
For the fungal colonisation subtype, the eradication or reduction of fungal and yeast colonies is usually recommended using herbal/natural and/or pharmaceutical antifungals. This may also involve biofilm eradication (biofilm busting) as these fungal/yeast colonies are often protected by biofilms.
Some protocols and doctors also aim to balance the nasal/sinus, oral, gut or skin microbiome(s) to improve a person’s external or internal microbiome terrain.
Indoor Environmental Professionals (IEPs) is a general term used to describe an individual with the knowledge and skills to be competent in a range of subjects related to mould in the built environment to quality them to perform assessments. In Australia, this may include Building Biologists, Occupational (Industrial) Hygienists, Mould Testing Technicians, and Mycologists/Microbiologists for example. According to the Australian Standard for mould remediation (AS-IICRC S520:2025, Standard for Professional Mould Remediation), an IEPs qualifications are gained through formal study in mould and the indoor environment at the tertiary level, and years of on-the-job work experience.
In the case of an insurance claim involving an escape of liquid event, the aim is to return the building and contents to the condition that the assessor feels was a reasonable estimate of pre-event condition. Whilst the approach of testing for mould may seem sufficient in for example a small escape of liquid within the last 24 hours, it must be remembered that mould is often present in wall cavities, behind cabinets, in roof voids and and other inaccessible places prior to the leak. This growth can be from an earlier event, high ambient humidity, or it may have been present at the time of initial construction (pre-existing damage). Upon becoming wet, the pre-existing mould can flourish. A person trained in understanding the visual, odour-based and invisible cues of mould growth is vital but so is the need to understand air movement, moisture mechanics and how a building design and assembly and its operation by its occupant should inform the investigation.
In the case of susceptible populations*, an IEP should be engaged who is independent from the remediator and builder conducting the rectification works. This Council recommends IEPs should be trained in the identification of the source(s) and the extent of water damage and microbial growth, location and boundary of fungal particulate spread (through sampling), ability to identify areas impacted by cross contamination (where applicable or possible), with the goal to establish the Condition of the materials and, where requested, contents in the built environment. This requires the ability to conduct an exposure history, undertake a thorough visual inspection for signs and sources of moisture and mould, water vapour management and moisture mechanics, impact of moisture on building material substrates, conduct moisture mapping, undertake sampling and interpret lab reports. We also acknowledge that whilst odour, visible mould, and elevated moisture are important markers of water damaged buildings, a significant proportion of homes that have not been impacted by recent water events, do not have any of these signs yet may expose the occupants to elevated fungal particulate that may increase the risk of adverse health effects. As such, sampling (air and surface) should be conducted to establish Condition 2 and 3 of the structure, contents and systems (HVAC), with a focus on areas frequently used by vulnerable occupants such as bedrooms and living spaces. An IEP should also have the skills to conduct a scope of remedial works required to return the property to an agreed condition.
*Susceptible populations include those based on age (young, elderly), those diagnosed with chronic conditions including asthma and allergies, and those who are immunocompromised.
Much of the mould growing on a material will frequently become airborne and settle onto new surfaces under gravity or get trapped in materials such as air filters and soft furnishings. The cycle of resuspension and settling of fungal material allows mould to move from its source at decreasing levels to multiple downstream surfaces that become secondary mould sources. Where humidity is high, mould can grow in the new location. Both scenarios allow mould to accumulate in locations that may not be routinely considered yet yield very high levels of inhalation exposure risk when disturbed. Examples include air filters in HVAC or portable air cleaners, carpets, curtains and the tops of high surfaces that face infrequent cleaning. It is therefore important that the professional chosen can fulfil the requirements of the AIHA/IAQA document and ASTM 7339:2014 – Standard for the Assessment of Fungal Growth in Buildings as it pertains to mould.
Please see the Mould and Building Inspection page.
Yes, ideally. An assessor who is independent from the mould remediator, should be engaged in any of the following scenarios:
- a preliminary determination indicates that mould contamination exists or is likely to exist,
- if confirmation of Condition is requested,
- if health issues are reported.
If the IEP conducting the assessment or PRV is not independent from the remediator, they should disclose in writing to the client that they are deviating from the Standard of Care.
The mould remediation contractor may undertake testing in situations where there are no health effects reported by the client OR where an entire building or system is fully involved as a result of Condition 3 mould contamination (for example after an extreme weather event), or when the scope of work can be determined without sampling.
Similarly, laboratories conducting sample analysis should remain independent of the person conducting the remediation and ideally independent of the site assessor. However, close contact and documented communication throughout the chain of contractors and services conducting all stages of remediation is critical in resolving health issues.
Note on Conflicts of Interest:
The American Council for Accredited Certification strongly discourages its certificants from performing both assessment services and contracting services on the same project. Certificants who offer both services to the same client create a perceived conflict of interest regardless of their integrity. Nevertheless, as circumstances sometimes prevent the employment of multiple professionals on the same project, ACAC does not prohibit the practice, nor does ACAC make compliance with this policy a condition of continued certification. ACAC code of conduct.
MAC does not favour one group of professionals over another for the investigation and remediation of water damage and microbial growth in buildings. Neither can we personally vouch for any of the professionals on the Mould and Building Inspection page — we recommend seeking referrals from previous clients, and conducting due diligence when selecting a professional.
| Question | Ideal response | |
| 1. | What are your qualifications? | Mycologists/Microbiologists
Building Biologist Certified Industrial Hygienist Mould Testing Technician IEP (other) |
| 2. | How long have you been doing this work? | At least 2+ years |
| 3. | Do you work independently from the remediator / builder? | Yes |
| 4. | How long does it normally take to inspect/test a 3 bedroom single storey home? | > 2 hours |
| 5. | What is the process you will undertake to test my home? | Exposure history, inspection, moisture mapping, thermal imaging, and sampling. |
| 6. | What type of sampling will you undertake? | Total spore count (air and surface) |
| 7. | Will I be given a comprehensive report outlining your findings and recommendations? Can you send me a sample report? | Yes |
| 8. | Do I need to do anything prior to you coming to test my home? | Yes, keep windows and doors closed for ~24 hours, and turn off air purifiers |
| 9. | Can you provide the contact details of 2 references? | Yes |
The Australian Standard for mould remediation is AS-IICRC S520:2025, Standard for Professional Mould Remediation. This standard has been derived from the Institute of Inspection, Cleaning and Restoration Certification (ANSI/IICRC S520 Standard for Professional Mold Remediation, 2024). IICRC offer certifications in mould remediation (www.iicrc.org.au).
Mould Illness/CIRS patients often require a more stringent level of remediation than that required by the IICRC standard. The Surviving Mold protocol to achieve this level is outlined in Schrantz, et. al. (2021) Indoor Environmental Professional Panel of Surviving Mold Consensus Statement for Microbial Remediation 2020. Medical Research Archives, 9(). https://doi.org/10.18103/mra.v9i1.2327
Please see the Mould Remediators page.
Questions you should consider asking a remediator prior to conducting the job:
| Question | Ideal response | |
| 1. | What are the qualifications of the person who will be undertaking the remediation? | IICRC |
| 2. | How long has this person been doing this work? | > 2 years |
| 3. | Is the IEP who will be conducting the pre and post remediation verification testing independent from you? | Yes |
| 4. | What methods do you use to remove mold? | HEPA sandwich, blasting, … |
| 5. | Do you recommend fogging or using biocides. If so, please provide Safety Data Sheets for those. | Fogging and biocides deviate from Standard of Care unless bacterial contamination is present |
| 5. | Will you set up containment and if so what does this involve? | Containment barriers, negative air machines, air scrubbers |
| 6. | Will you inspect my home and give me an itemised quote prior to conducting the remediation? | Yes |
| 7. | Does the quote include remediating my contents? How will you do this? | Yes |
| 8. | Will I be given documentation (scope of works) regarding what will occur in my home? | Yes |
| 9. | Can you provide the contact details of 3 references? | Yes |
Yes where feasible, independent assessors, remediation contractors and laboratories with no financial links, including through a parent company, are recommended. Communication throughout the chain of contractors and services is critical in securing the best outcomes. See Part 7.3 of this FAQ for more detail.
Please see the Mould 101 – Preventing, Removing and Remediating page.
You must be logged in to post a comment.